


Surgery for glaucoma is always the last resort. It usually means we have tried all forms of medication and other non-invasive methods to control eye pressure and nothing has been successful. Glaucoma surgery, while successful, also comes with risks. These risks can range from mild to severe. The common risks associated with all surgeries such as swelling, bleeding, and infection can also be associated with glaucoma surgery. However, if any of these happen to the eye, it is especially devastating causing a loss of vision, and these complications are often hard to treat.
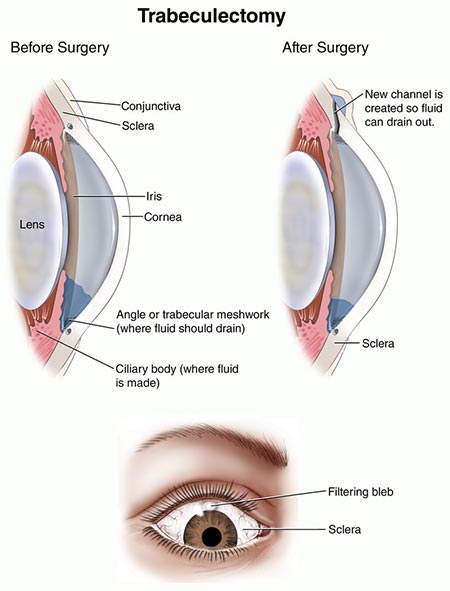
The gold standard for glaucoma surgery is called a trabeculectomy. During this surgery, the surgeon creates a pathway for the fluid in the eye to drain to the outside of the eye, under the skin (conjunctiva) of the eye. We call this drainage reservoir a “bleb.” As you can imagine this surgery is very tedious and precise in order to have a successful outcome. It requires lots of eye drops and restrictions for several weeks to months after completed. This surgery is very successful but still not 100% effective.
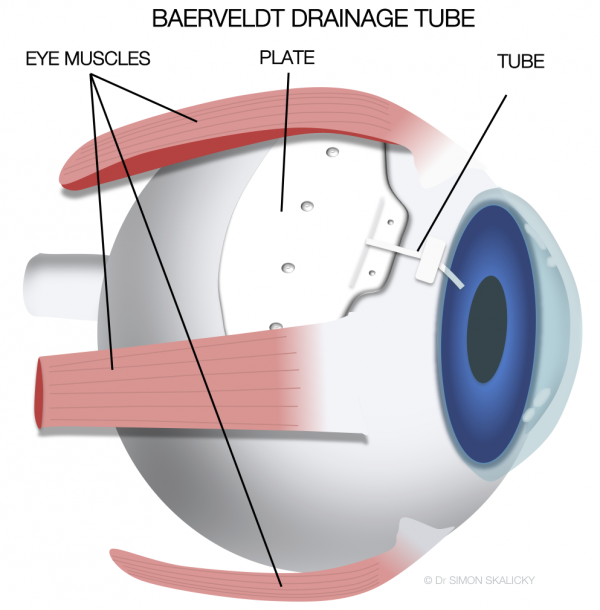
If more advanced glaucoma is present or a trabeculectomy has been unsuccessful another option is something called a tube or shunt surgery. With this surgery, a device called a Molteno, or Baerveldt, or Ahmed valve is implanted partially inside the front of the eye and partially outside the eye under the upper eyelids. Patients don’t feel this implant but it can be seen if the patient looks in a far downward direction. This type of surgery has become much more popular in recent years. This type of tube or shunt surgery is very good at lowering pressure but requires a lot of post-operative monitoring and care as it is considered an invasive surgery.
A relatively new surgical category that has been gaining ground is called MIGS or Micro-Invasive Glaucoma Surgery. I’ll talk more about that in another session.





