


We are very happy when one of our own does something good and important.
Many remember when Dr Gribble/Wong was with us a few years back, and you remember how sad we were to see her go. After The Eye Center, she moved to Atlanta and added a second fellowship (Retina) to her Ophthalmology and Ocular Uveitis expertise. She is now a partner with Eye Consultants of Atlanta, and still acts as a consultant for usual and difficult cases.
Recently Margaret was lead author on a report about a serious case of eye cancer, which they were able to successfully treat. This was published in the January 2022 issue of the prestigious American Journal of Ophthalmology Case Reports. One of her co-authors was Carol Shields of the Wills Eye Hospital of Thomas Jefferson University medical school. Carol and Wills Eye are world famous and greatly respected for their work in the diagnosis and treatment of ocular cancers.
Well Done Margaret!
Non-small cell lung cancer with iris metastasis controlled with osimertinib and monthly intravitreal bevacizumab
Margaret Wong, James H. Frank, and Carol L. Shields
Purpose: Iris metastases from lung cancer occur rarely. Current treatment options such as surgical iridectomy or radiotherapy are invasive and can potentially lead to negative side effects. Other less invasive alternatives include chemotherapy and intracameral bevacizumab.
Observations: An 81 year-old female with metastatic non-small cell lung adenocarcinoma to the iris in the right eye was treated with daily oral osimertinib 80mg, an epidermal growth factor receptor (EGFR) tyrosine kinase inhibitor (TKI), for her systemic lung cancer. In addition, 8 monthly intravitreal bevacizumab (1.25mg/0.05 cc) injections were given. The iris tumor demonstrated complete regression by the third cycle of osimertinib. Following 21 months of osimertinib and 8 bevacizumab injections, the tumor remained regressed. Subsequent iris biopsy confirmed complete tumor regression.
Conclusions and Importance: In this case, osimertinib and monthly intravitreal bevacizumab controlled iris metastasis due to non-small cell lung cancer. Osimertinib can be beneficial for patients with EGFR-positive lung cancer for both ocular and systemic control.
Introduction
Uveal metastases from systemic tumors can occur, most often from primary breast or lung cancer. According to Shields et al., of all uveal metastases, only 8% involve the iris.1 Further, of patients with primary lung cancer in that series (n = 336 patients), iris involvement with metastases was found in 9%.1 In recent years, cancer patients have shown improved lifespan, especially with newer chemotherapies and immunotherapies. Current treatments for iris metastasis from systemic cancers include systemic chemotherapy, external beam radiotherapy, plaque radiotherapy, sur-gical excision, enucleation, and observation. In one analysis of 104 consecutive patients with iris metastasis, 27% of these tumors arose from cancer of the lung.2 In that series, treatments included systemic chemotherapy (22%), external beam radiotherapy (41%), plaque radiotherapy (24%), surgical excision (5%), enucleation (4%), or observation (5%).2 When considering therapy for non-small cell lung cancer (NSCLC), epidermal growth factor receptor (EGFR) is an important target as those who test positive for this mutation are suitable for treatment with EGFR tyrosine kinase inhibitor (TKI), including medications such as erlotinib, gefitinib, or afatinib.3–5 This class of chemotherapy has been especially effective in treating EGFR-positive primary lung cancer and the related uveal, specifically choroidal, metastases.6–8 However, NSCLC patients can develop resistance to first- and second-generation EGFR-TKIs.9 Osimertinib is a third-generation EGFR-TKI and has been successfully used in the treatment of NSCLC that have acquired resistance to first- and second-generation EGFR-TKIs.10 Osimertinib has not been docu-mented, as of yet, for control of iris metastases associated with NSCLC, although it does show efficacy in treatment of choroidal metastases in two case reports.11,12 Additionally, several reports have identified bev-acizumab intraocular injection as a potential treatment option for iris metastases secondary to lung cancer. Support of bevacizumab usage is found in mice with NSCLC and overexpression of vascular endothelial growth factor (VEGF)-A.13 There are 3 published human case reports documenting bevacizumab efficacy for iris metastasis.14–16 Herein, we describe a patient with iris metastasis from NSCLC who showed a complete response to combination osimertinib and intravitreal bevacizumab.
Case Report
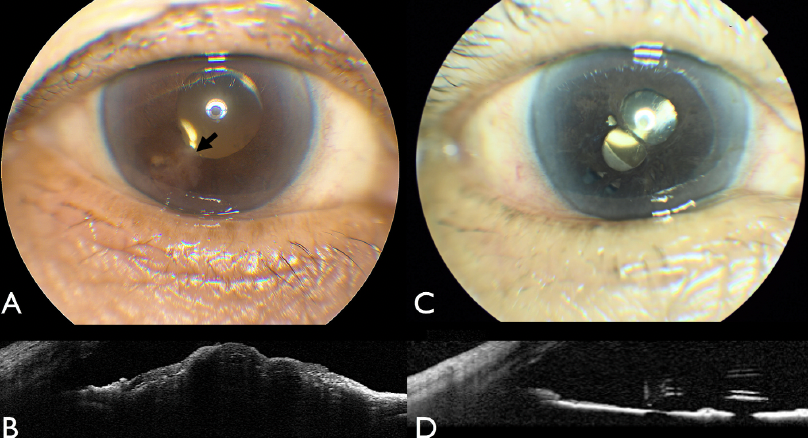
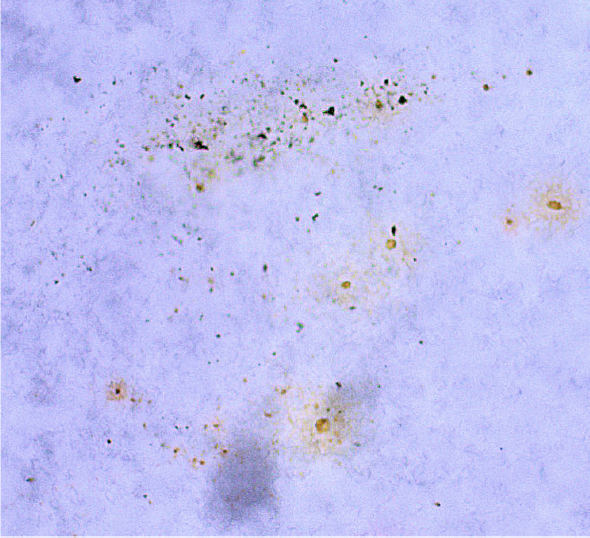
An 81 year-old female noted gradually worsening blurred vision and pain in the right eye (RE) for 1 month. Pertinent review of systems was positive for 3 months of back pain that led to a diagnosis of stage 4, NSCLC, EGFR-mutation positive with metastases to the ribs, third thoracic vertebra, and brain. Past ocular history revealed dry macular degeneration. The patient was urgently started on oral osimertinib 80mg daily 4 days prior to ophthalmic presentation. On examination, best correct visual acuity was 20/60 RE and 20/40 left eye (LE). The pupillary reaction, extraocular motility, and confrontation visual fields were normal. Intraocular pressures were 13 and 14 mmHg, respectively. Slit lamp examination of the RE showed trace cells in the anterior chamber and there was a non-pigmented, grey- white mass on the iris inferotemporally with ill-defined margins, measuring 5 mm in diameter (Fig. 1A). There were several satellite le-sions. The anterior vitreous was clear. The LE anterior segment was normal. On gonioscopy RE, the angle was open and there was no infiltration. Fundus examination of each eye showed features of macular degenera-tion with bilateral intermediate drusen and no sign of choroidal mass. Imaging with anterior segment optical coherence tomography (AS- OCT) documented a multinodular optically dense iris mass with poste-rior shadowing, suggestive of tumor (Fig. 1B). Given her history of NSCLC, the patient requested the least invasive treatment approach. Options included radiotherapy, iridectomy, or continuation of the osimertinib with additional intravitreal bev-acizumab injections. The latter approach was chosen and following 1 cycle of osimertinib initiation, there was substantial tumor reduction on examination and AS-OCT. Daily osimertinib administration can be divided into 21-day cycles. By 3 osimertinib cycles, the tumor showed complete regression and this was confirmed on AS-OCT. By 5 osimerti-nib cycles, tiny cysts appeared in the area of initial tumor, confirmed on AS-OCT. Following 7 cycles, the iris cysts increased in number, and were located on both the temporal and nasal sides of the iris. Following 8 osimertinib cycles, the appearance of iris remained the same. The exam and AS-OCT at this point showed multiple iris cysts and no signs of tumor, and the monthly bevacizumab injections were stopped. The most recent follow up was 21 months after initial presentation with contin-uous daily dosing of osimertinib, which showed complete control on examination (Fig. 1C) and AS-OCT (Fig. 1D). A decision was made to perform a fine needle biopsy of the iris cysts and aqueous fluid, which revealed non-carcinoma debris (Fig. 2). The most recent visual acuity RE was 20/40. The patient denied ocular side effects from therapy and is currently in systemic remission of the NSCLC with continuous daily osimertinib dosing.
Discussion
Herein, we describe a patient with iris metastasis from NSCLC adenocarcinoma that was successfully controlled with continuous daily dosing of oral osimertinib and 8 monthly intravitreal bevacizumab injections. Osimertinib is a third generation EGFR-TKI, effective for treatment of NSCLC in patients with an EGFR mutation.17 The EGFR activation of intracellular tyrosine kinase activity leads to tumor proliferation by way of angiogenesis, inhibition of apoptosis, and spread of tumor cells.17 Inhibition of this cascade of events illustrates the mechanism of efficacy of EGFR-TKIs against NSCLC.17 Patients with the EGFR mutation respond more favorably to the EGFR-TKI class of medications, compared to those who do not have the mutation.18 Patients with NSCLC treated with EGFR-TKI show 12-month survival rate of 82% if EGFR-mutation-positive versus 63% for those who are EGFR-mutation-negative.18 Therefore, it is important to test patients for this mutation to improve the efficacy of the chemotherapy.
In addition, the characteristics of NSCLC adenocarcinoma type, non-smokers, and female gender also increase the efficacy of the medi-cation.18 Our patient demonstrated all of these characteristics, a boost for the overall outcome in this case. Not only is this class of chemotherapy effective against the primary tumor, it can be effective for related metastasis. In the literature, our team described a patient with NSCLC and choroidal metastasis that showed robust response to erlotinib, a first-generation EGFR-TKI.6 Kim et al. described regression of choroidal metastasis from NSCLC following erlotinib and 3 intravitreal bevacizumab injections.7 Matura et al. showed reduction in choroidal metastasis following gefitinib, a first-generation medication, plus 4 monthly intravitreal bevacizumab injections.8 There are other single-case reports of similar choroidal metastasis control with EGFR-TKI, but our case is the first to document control of iris metastasis with this class of medication. Similarly, iris myeloid sarcoma secondary to acute myeloid leukemia can show regression with gilteritinib, another class of TKI targeting of the FMS-like tyrosine kinase 3.19 It is known that NSCLC can develop resistance to first- and second- generation EGFR-TKIs.9 Resistance can be acquired through the devel-opment of the T790 M mutation in the EGFR receptor.9 In such cases, testing for T790 M mutation may lead to opportunity for more potent third-generation EGFR-TKI, like osimertinib.10 There have been 2 cases describing complete regression of choroidal metastasis from NSCLC using osimertinib alone.11,12 With regards to bevacizumab, several case reports have shown regression of iris metastases secondary to lung cancer following bev-acizumab injections, but all with limited follow up.14–16 Schell et al. described a patient with NSCLC iris metastasis with regression following one intracameral bevacizumab injection and 2-month follow up.14 Other cases describe multiple iris metastases from small cell lung cancer and non-keratinizing squamous cell lung cancer, each showing tumor reduction following one intravitreal bevacizumab injection and only 1-month follow up.15,16 Based on the results of these case reports, we added monthly intravitreal bevacizumab to our patient’s treatment regimen hoping to improve the success of tumor regression with the addition of local therapy to the eye. We chose the intravitreal route of delivery instead of intracameral because bevacizumab remains longer in the vitreous humor compared to the aqueous humor, which has a much more rapid turnover rate.20 We stopped after 8 injections following the disappearance of tumor on exam and AS-OCT. The timing of monthly bevacizumab injections was based on pharmacologic studies where it was shown that significantly elevated levels of bevacizumab levels in the vitreous lasted approximately 30 days post intravitreal injection.21 While the intravitreal bevacizumab played a role in tumor regression in our case, we believe osimertinib had a greater effect compared to bev-acizumab, given the robust data showing systemic and ophthalmic tumor control with EGFR-TKIs. To our knowledge, this is the first case of biopsy-proven, iris metastasis regression from NSCLC following treatment with osimertinib and intravitreal bevacizumab, and also the longest follow up (21 months) for this tumor type. With regard to the iris cysts, it is unclear what caused the formation of the cysts or their significance, and we speculate they could represent necrotic remnants of tumor that dis-appeared by most recent follow up. It is unclear from this single case whether individual osimertinib or individual bevacizumab treatment could result in tumor control or regression. Perhaps a randomized controlled trial comparing osimertinib alone versus monthly bev-acizumab alone versus osimertinib plus monthly bevacizumab could answer this question. However, given the rarity of this type of tumor, it may be impossible to perform this type of study.
Conclusion
We report successful treatment of iris metastasis from NSCLC (EGFR- mutation-positive) with continuous daily oral dosing of osimertinib and monthly intravitreal bevacizumab without tumor recurrence after long- term 21 months follow up. While other treatments can be offered, this systemic therapy can control both the ophthalmic and systemic metastasis.




